AI-powered “smart patient retrieval” could transform tumor board decision-making
AI figure developed by Katelyn Lu, University of Michigan
3–4 minutes
AI figure developed by Katelyn Lu, University of Michigan
Tumor boards are a cornerstone of cancer care, with oncologists, radiologists, pathologists and other specialists collaborating to interpret complex evidence and recommend treatment. But as precision oncology evolves, so does the workload: expanding genomic panels, multimodal imaging, pathology findings and long treatment histories can make it difficult to assemble a complete picture quickly—especially when the most challenging cases are the ones that most need careful deliberation.
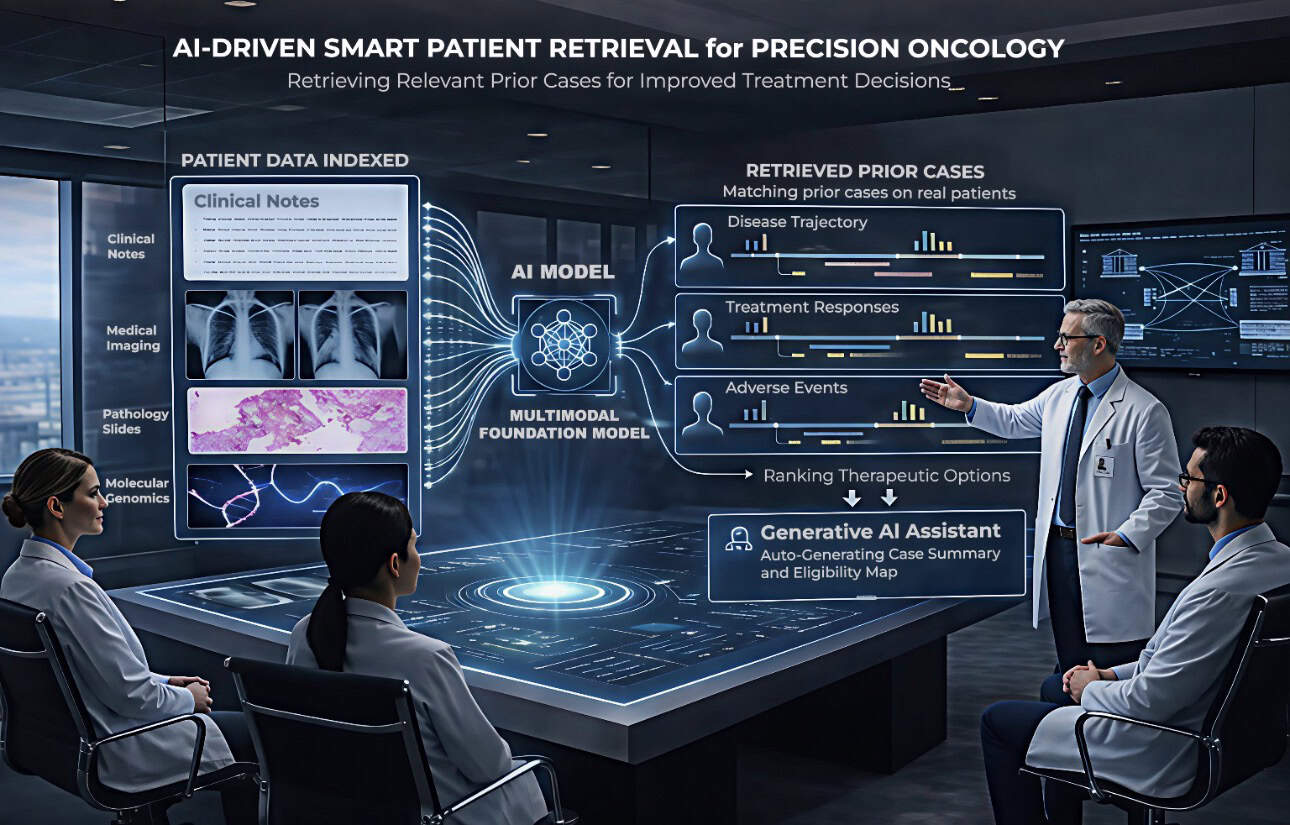
In a new perspective published March 26, 2026, in Nature Reviews Cancer, Joyce Yan-Ran Wang, Assistant Professor, Biomedical Engineering, and the study’s corresponding author, makes the case for a complementary AI capability designed to support these multidisciplinary decisions: AI-driven smart patient retrieval. The article, “AI-driven smart patient retrieval for precision oncology,” posits that oncology teams could benefit from systems that retrieve prior patients who are clinically similar to the current patient—and pair those matches with real-world treatment trajectories and outcomes.
Dr. Wang and the co-authors use the term “smart patient retrieval” to describe semantic multimodal retrieval systems that learn joint representations across clinical records, medical images, pathology and molecular data. Rather than relying on keyword searches or rigid structured filters, these systems aim to recognize similarity distributed across different data types—for example, where subtle imaging patterns, text-documented symptoms and combinations of molecular alterations together signal clinically meaningful resemblance.
“This is essentially a call to action,” Dr. Wang said. “We think this is a very important and promising way to achieve real precision oncology. This AI system not only looks at the image, but also looks at multimodality information, including imaging such as radiographic imaging, CT scan and pathology data, as well as genetic information. So this is designed to integrate all of the past information with new data and identify the most similar cases that can provide insightful information for new patients.”
The approach formalizes a common reasoning pattern in oncology—“I had a similar patient who…”—and scales it beyond any one clinician’s personal experience. That matters because, in rare cancers and unusual tumor presentations, even seasoned specialists may encounter only a handful of comparable cases over an entire career. Smart retrieval could help surface relevant historical cases across a health system or network of institutions, expanding access to collective knowledge.
The authors also highlight potential patient-facing impacts. Trial matching and therapy selection are often constrained by narrow rule-based criteria that focus on a small set of biomarkers. Smart patient retrieval could broaden the search by incorporating unstructured notes and multimodal signals, potentially helping identify patients with rare mutations or atypical profiles who might otherwise be missed—an especially important consideration for improving equitable access to advanced therapies and clinical trials.
At the same time, the article emphasizes that clinical deployment requires careful design and validation. “Similarity” in an AI model does not automatically translate into clinical relevance, and retrieved outcomes reflect real-world treatment patterns rather than controlled experiments. The authors outline research directions such as outcome-aware representation learning, two-stage retrieval that first enforces hard clinical constraints, and clinician feedback to align results with expert judgment. They also call for strong safety and governance practices, including human-in-the-loop review, uncertainty estimation, bias assessment and audit trails.
“We advocate for coordinated action,” Dr. Wang said. “The academic centers should digitalize these tumor board workflows and also like clinicians must be engaged as co-designers because their clinical judgment is a critical component of the system. This is a collaborative effort and a collective commitment to think about how we can make the best use of the data and AI model to improve cancer care.”
Dr. Wang and colleagues further argue that large language models could support tumor board workflows when grounded in retrieved evidence—helping generate structured case summaries and synthesize multimodal patient data without drifting into unsupported claims.
Overall, the perspective offers a roadmap for how AI could help tumor boards move from time-consuming data-gathering toward more focused, evidence-informed discussion—anchored not only in guidelines and literature, but also in what happened to actual patients whose treatment data and disease experiences can benefit others.